
Cannabis is an extremely ancient drug. Its widespread use is mentioned in the earliest Chinese pharmacopeias as well as the Rig Veda and Avesta, the founding texts of Hinduism and Zoroastrianism respectively. Many uses are listed for the drug including beneficial effects on pain, inflammation and a variety of psychiatric problems. Indeed, the Avesta says that cannabis is the most useful of all known drugs. Cannabis has been used in Asia for medical purposes for thousands of years. The drug eventually arrived in Europe by various routes including being brought back from Egypt by Napoleon’s troops and by the British such as Dr. William O’Shaughnessy from the British Raj in India. From Western Europe cannabis spread to the United States where it was beloved by people such as the writers Fitzhugh Ludlow and Louisa May Alcott. Throughout the 19th and early 20th centuries cannabis was widely appreciated in Europe and America for its medical properties. Cannabis tinctures were sold by most of the major European and American drug companies and it was a component of many patent medicines.
But then something happened. The 19th century saw the first attempts to regulate and tax the distribution of drugs. The introduction of heroin (marketed by the Bayer company in 1898) and the appearance of heroin addiction in the first decades of the 20th century, as well as increased use of opiates by the military and addiction to purified cocaine, resulted in the first international attempts to legislate the trade and use of highly addictive substances. In the USA the result was the Harrison Tax Act of 1914. Eventually the US government set up the Federal Bureau of Narcotics (FBN) in 1930 which was supposed to have overall control of drug issues. Their choice of the man to run the FBN, Harry Anslinger, was an unfortunate one. Political issues and corruption made it difficult for Anslinger to pay much attention to illegal heroin operations. So, in order to provide some kind of rationale for the Bureau’s activities, Anslinger decided to turn his attention to the use of cannabis. The drug had now become widely known by its Spanish name “marijuana” because it was used by immigrant Mexican workers with little political influence. Through the use of a spectacularly ridiculous “fake news” campaign, Anslinger spread the idea that cannabis/marijuana was actually the most dangerous substance in the world and that its use was the trigger for an enormous number of serious criminal activities, including rape and murder. In reaction to all of this, strict laws were passed restricting the availability of cannabis and its use for any sort of respectable medical purpose completely disappeared. The eclipse of cannabis was absolute.F
The situation began to change in the 1960s when cannabis use became associated with the very lively counterculture movement. Gradually “grass roots” organizations began to agitate for the legalization of cannabis once again. These efforts have met with increasing success in the 21st century and now cannabis use is legal for medical or recreational purposes in many parts of the USA as well as in several other countries such as Canada and Uruguay. There is every indication that this trend will continue to expand in the coming years. There is now a vigorous discussion as to which of the many claims concerning the health benefits of cannabis are actually true as a whole new generation begins to rediscover things that humanity has really known for thousands of years. Of course, the societal context for cannabis use has now changed somewhat and advances in science and technology are able to make more sophisticated judgements as to cannabis’ true medical potential.
Really the debate about cannabis concerns the properties of the two major pharmacologically active chemical components of the cannabis plant -the “phytocannabinoids” tetrahydrocannabinol (THC) and cannabidiol (CBD). Although they are related chemically, these two molecules have very different properties. As we shall discuss, THC is responsible for the known psychoactive effects of cannabis as well as several of its well-established pharmacological effects. CBD, on the other hand, is devoid of psychotropic properties. Generally speaking CBD has been viewed by regulatory agencies as being much less “dangerous” than THC. Because CBD is now widely available there are a huge number of claims as to its health benefits, many of which are undoubtedly spurious. Nevertheless, it appears that CBD does produce some interesting pharmacological effects (e.g. in the treatment of childhood epilepsies). Unfortunately, there is no real understanding as to how CBD works in terms of a molecular mechanism ,making it difficult to really evaluate it.The situation with THC is quite different. Here there is a very well described molecular context for understanding the mechanism of action of the drug, meaning that the basic tools of pharmacology can be brought to bear on refining any potential health benefits it might produce. Indeed, these benefits have recently been highlighted in a spectacular manner.
In order to understand these new revelations we should first briefly discuss what is known about the mechanism of action of THC. Like most drugs with well understood mechanisms, THC acts by interacting with a receptor-or actually two receptors. These are known as “cannabinoid” receptors-the CB1 and CB2 cannabinoid receptors. Both of these are what are known as G-protein coupled receptors, which constitute the largest family of receptors and one of the largest families of proteins in the genome. THC acts as a partial agonist at cannabinoid receptors. CB1 receptors are very highly expressed in the nervous system, whereas CB2 receptors are more highly expressed in cells like white blood cells. Of course, cannabinoid receptors do not exist in nature just to mediate the effects of THC. In reality, they are the receptors for what are known as “endocannabinoids”, endogenous substances that are found in all animals and which normally activate CB1 and CB2 receptors. In the brain, for example, endocannabinoids act as neurotransmitters that carry information from one nerve cell to another.
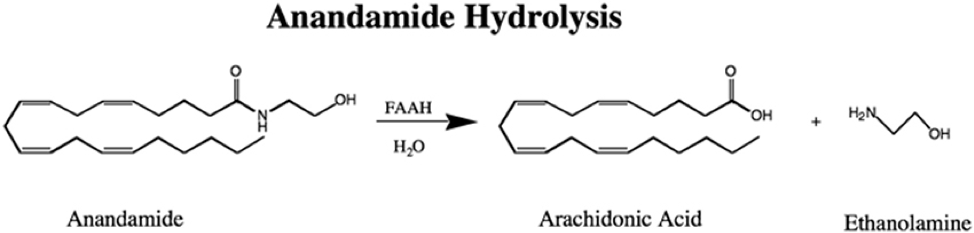
Now that the potentially useful pharmacological effects of THC have been “rediscovered”, there is a great deal of interest in making synthetic cannabinoids that stimulate or inhibit cannabinoid receptors for treating different disease states including pain, inflammation and nausea associated with chemotherapy. But, of course, in principle there is another way to achieve these same effects. What if you could make your body raise its own levels of endocannabinoids? This should produce a similar effect to giving a drug that activates cannabinoid receptors. Indeed, such an approach is certainly possible in principle. The two major endocannabinoids are known as anandamide and 2-arachidonoyl-glycerol (2-AG). They are derivatives of a molecule called arachidonic acid which is known to play a central role in many biologically important processes. The two endocannabinoids are synthesized and destroyed by specific enzymes. For example, the enzyme that destroys anandamide is called Fatty Acid Acyl Hydrolase (FAAH). Supposing we had a drug that inhibited this enzyme. The result might well be that levels of anandamide would rise because it is no longer being destroyed efficiently and this would result in increased activation of cannabinoid receptors. This kind of approach has many precedents in pharmacology. For example, if we believe that biogenic amines like norepinephrine and serotonin are important for the maintenance of normal mood, then raising their levels might be good for treating depression. As these substances are normally destroyed by the enzyme monoamine oxidase (MAO), then a drug that blocks the activity of this enzyme should raise biogenic amine levels and counter depression. This turns out to be broadly true-monoamine oxidase inhibitors like iproniazid were the first successful antidepressant drugs. Blocking FAAH to raise levels of anandamide would be an equivalent procedure.
As the biology of endocannabinoids became clearer many drug companies were attracted to the idea that FAAH antagonists might be useful drugs. Take pain, for example. We all know that treating chronic pain with opiates produces addiction -that’s why we have an opioid crisis at the moment. Because we know from much historical and recent evidence that activation of CB1 receptors might be helpful for pain, maybe a FAAH antagonist would be good for this purpose, making it a really useful new drug ?
So, the race was on. Several big pharmaceutical companies such as Pfizer produced a range of potent FAAH inhibitors. Another company that was in the game early on was a Portuguese drug company called Bial. The company began a series of preclinical trials on its new compounds and picked a drug called BIA 10-2474 as its lead molecule for further development. After conducting a series of tests the company decided that the drug seemed promising enough to begin clinical trials in humans. Human trials usually begin with “Phase 1” trials that are run to assess the general safety of the new compound and to collect some basic data on drug metabolism. In order to carry out this trial Bial hired an experienced company in Rennes, France, named Biotrial Research that uses hospital facilities at Rennes University for carrying out trials such as these. Six doses of BIA 10-2474 were to be tested on human volunteers – 2.5 mg; 5 mg; 10 mg; 20mg; 50 mg and 100 mg. Each dose was to be administered for 10 consecutive days. Nothing untoward was expected. But things didn’t go according to plan. In fact the trial was a complete disaster. On the evening of day five (10 January 2016) and the fifth administration of the 50 mg dose, the highest dose category tested at that point, one of the 6 volunteers who had received the drug rather than the placebo had to be hospitalized in serious condition. This patient sank into a coma and died. Four of the other five men in the same dosage group were also hospitalized between 10th and 13th of January displaying similar symptoms to those of the man who died. The symptoms experienced by the affected participants were all of a neurological nature resembling those associated with a stroke. These included severe headaches and problems with consciousness ranging from sedation to coma and memory impairment. The trial was immediately abandoned. The four hospitalized patients that didn’t die all eventually survived, although several of them had severe symptoms over an extended period of time. Brain imaging studies demonstrated that these individuals had several structural anomalies in their brains strongly suggestive of a toxic or metabolic mechanism for the adverse effects of the drug.
A subsequent investigation as to the causes of the fiasco revealed several interesting things. As it turned out BIA 10-2474 wasn’t a very good FAAH inhibitor, particularly when compared to other clinical candidates that had been produced by the likes of Pfizer and Johnson and Johnson. The potency of the drug wasn’t very high and its selectivity, that is its propensity to act on FAAH rather than other targets, also wasn’t that clear. It appears that the animal testing done by Bial with respect to effects on pain, the supposed major endpoint to be examined, was rather rudimentary and the doses calculated for use in humans were based on animal experiments which turned out to be misleading. A key question was whether the toxicity of the drug was due to its effects on FAAH or due to other “off target” effects resulting from its lack of specificity. Without going into all of the evidence , it seems most likely that the latter alternative was the correct one. Nevertheless, it was not surprising that ongoing programs at other drug companies to develop clinically effective FAAH antagonists came to an abrupt halt. The idea that this might be a route for the production of a novel analgesic drug seemed dead as a doornail…or was it?

About 6 years ago Mrs. Jo Cameron, a woman living in Inverness in Scotland, came to her local hospital with severe osteoarthritis of the hip. Interestingly, Mrs. Cameron didn’t seek medical help because her arthritis hurt -it didn’t. Rather she was having mechanical issues resulting from hip degeneration. Asked if she needed pain killers following her hip replacement, she declined. A year later she was back in the hospital for an operation on her hand. Once again she said she didn’t need pain killers. Needless to say the doctors involved were puzzled by Mrs. Cameron’s lack of pain under circumstances in which other people invariably report extremely severe pain. On investigating Mrs. Cameron further several other interesting facts about her came to light. She had quite extensive scarring resulting from an abnormally large number of previous injuries from burns, cuts and other types of trauma. As it turned out she was frequently unaware when her skin was burning, only being alerted to the situation by the smell of burning flesh rather than any pain. Mrs. Cameron also told the doctors that the birth of her two children had not been painful at all. She had felt some stretching sensations but no discomfort. All in all she thought that the experience had been a uniformly pleasant one. The doctors then asked Mrs. Cameron if she would eat a habanero chili pepper. Habanero or Scotch Bonnet peppers are among the world’s hottest. No human being can just pop one in their mouth, chew it and swallow it without experiencing excruciating pain. But Mrs. Cameron could do it with no trouble at all, merely remarking that the habanero produced a nice warm feeling in her mouth. Another curious thing about Mrs. Cameron was that she had a remarkably calm, mellow and cheerful personality. When given questionnaires to assess her levels of anxiety and depression, she scored zero on each of them. Finally, Mrs. Cameron declared that she frequently forgot things like where she had put her keys. One can watch Mrs. Cameron discuss these matters live on You Tube:
It’s a remarkable performance. Overall, one might be forgiven for thinking that Mrs. Cameron was continually high on cannabis. Because of Mrs. Cameron’s resistance to pain, together with her unusually equanimous personality, the doctors referred her to the Molecular Nociception group at University College in London for a genetic assessment. The surprising results of this investigation were recently published (Habib et al 2019). The bottom line is that Mrs. Cameron has some interesting mutations in her FAAH gene. In fact, Mrs. Cameron has a very unusual genetic profile indeed. The first thing that the investigators discovered was that right next to the FAAH gene was a FAAH “pseudogene”. This is a fairly common occurrence in the genome when a gene is duplicated and the sequence of one copy starts to drift so that it no longer has its original protein coding function. Nevertheless, some pseudogenes have attained new functions concerned with different sorts of gene regulation. The scientists investigating Mrs. Cameron dubbed the new pseudogene “FAAH-OUT”. It appears that Mrs. Cameron carries a microdeletion of genetic material that has removed the promoter region and the first two exons of the FAAH-OUT gene. For some reason, this deletion has not only crippled the FAAH-OUT gene but also the FAAH gene, indicating that the expression of FAAH is normally controlled by some function of FAAH-OUT, although precisely what that function might be remains speculative at this time. Of course, every human carries two copies of each gene (alleles). Although the production of FAAH by one of Mrs. Cameron’s alleles seems to have been crippled, she also has another allele that might well compensate for this loss. But, fascinatingly, in Mrs. Cameron’s case, the situation is different. It is well known that every gene contains small changes in nucleic acid sequence throughout the human population. These are called single nucleotide polymorphisms or “SNPs”. Sometimes these changes make no difference whatsoever, but in other instances they may increase or decrease the activity of the gene. Just as with all genes, there are numerous SNPs in the human FAAH gene, some of which produce a “hypomorphic” phenotype, meaning that the gene functions less well. As things turn out, Mrs. Cameron’s second allele carries a FAAH gene with a missense variant converting proline at position 129 to threonine (rs324420). This has been shown to result in lower FAAH activity and is associated with significantly lower pain sensitivity and less need for postoperative analgesia. Hence, Mrs. Cameron carries two alleles that produce deficient FAAH function. That being the case one would expect Mrs. Cameron to have abnormally high levels of the endocannabinoid anandamide which is normally a substrate for FAAH. This was exactly what was found to be the case. Interestingly, Mrs. Cameron’s son carries the gene microdeletion but not the SNP and Mrs. Cameron’s mother carries the SNP but not the microdeletion. Both of these individuals have some pain hyposensitivity but it is not nearly as marked as that displayed by Mrs. Cameron who carries both dysfunctional alleles.The results of these studies have important implications for cannabis pharmacology. Mrs. Cameron can be viewed as an experiment carried out by Nature.In effect it is an experiment carried out in a human rather than in mice where pharmacological results are frequently misleading. The data appear to suggest that drugs that inhibit FAAH activity might well have useful properties. In particular, if Mrs. Cameron is anything to go by, they may have beneficial effects on pain and mood, two areas of pharmacology where new drugs are urgently needed after little progress in these fields for many decades. Moreover, it also appears that, in addition to FAAH itself, FAAH-OUT may be a novel drug target-although a great deal more work is required before we understand exactly how this gene operates. It appears that the unfortunate results of the BIA 10-2474 trial may in fact be something of a red herring and that now the pharmacological industry might consider reinvesting in this area, even though it has not previously yielded promising clinical results.
The results of the FAAH-OUT investigation also tell us that the interregnum of the last 70 or so years when the use of cannabis has been severely restricted, for what are clearly political reasons, was a medical mistake. History assures us that attention to the medical properties of cannabis will surely yield useful results in the future.
FURTHER READING
Microdeletion in a FAAH pseudogene identified in a patient with high anandamide concentrations and pain insensitivity. Habib AM, Okorokov AL, Hill MN, Bras JT, Lee MC, Li S, Gossage SJ, van Drimmelen M, Morena M, Houlden H, Ramirez JD, Bennett DLH, Srivastava D, Cox JJ. Br J Anaesth. 2019 Mar 28. pii: S0007-0912(19)30138-2. doi: 10.1016/j.bja.2019.02.019. [Epub ahead of print]. PMID: 30929760